Chapter 5: Managing Fracture and Dislocation
Nazrin Ahmad and Rosnah Majin
Learning Objectives
Type your learning objectives here.
- Define what immobilisation is.
- Recognise types of fracture and dislocation.
- Perform techniques to manage fractures and dislocations.
5.1 Introduction to Immobilisation
Immobilisation is a method used to restrict the movement of bones or joints to manage fractures and dislocations. It refers to the process of stabilising an injured limb to protect surrounding tissues and organs during the immediate post-fracture phase. The primary objectives are to prevent further injury, alleviate pain, and, in some cases, assist in controlling bleeding. Various techniques can be applied depending on the site of the fracture or dislocation. The effectiveness of immobilisation often depends on the type of equipment used or adaptations made to the technique. These methods may range from basic to advanced, depending on the first aider’s level of skill. In certain situations, immobilisation may also be combined with bleeding control measures to preserve life.
5.2 Types of Bone Fracture and Dislocation
A fracture is a break or crack in a bone that occurs when an external force exceeds its strength, leading to either a partial or complete break. It may result from trauma such as falls or accidents, repetitive stress, or underlying conditions like osteoporosis, with causes including direct impact, twisting forces, compression, or pathological weakening. Fractures are classified as open, where the broken bone protrudes through the skin and may cause severe bleeding, or closed, where the deformity is evident without bone exposure. A dislocation, on the other hand, happens when the ends of bones in a joint are forced out of their normal position, disrupting joint alignment and often injuring surrounding ligaments, tendons, and soft tissues. It is typically caused by sudden impact, falls, sports injuries, or forceful twisting, with common sites including the shoulder, elbow, fingers, hip, knee, and jaw. Both fractures and dislocations share similar signs, including severe pain, swelling, deformity, restricted movement, and occasionally numbness due to nerve compression. Therefore, FA management for both conditions primarily involves immobilisation.

5.3 Different types of immobilisation and their indications
a) Arms sling application
Arm sling application refers to the procedures of applying a triangular bandage or specialised sling to support the forearm and hold the arm in a comfortable and secure position across the chest. This procedure is performed to immobilise fractures, dislocations, or soft tissue injuries of the upper limb. The aim is to restrict movement of the arm, shoulder, or wrist, reduce pain, minimise the risk of further injury, and promote comfort and healing until definitive medical treatment is provided.
The indications for arm sling application:
- Fractures of the arm, forearm, collarbone (clavicle), or shoulder.
- Dislocations of the shoulder or elbow.
- Soft tissue injuries of the arm.

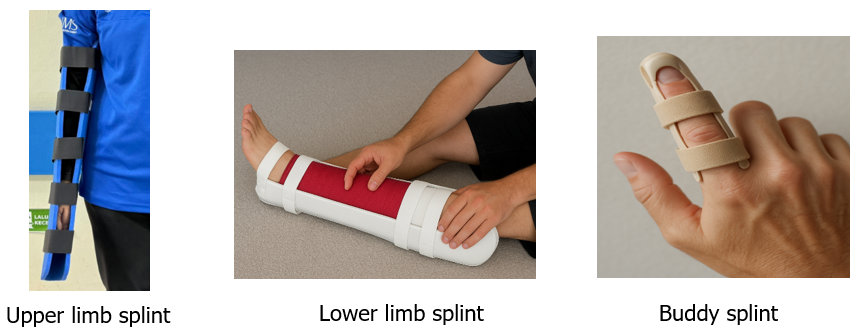
b) Splinting
Splinting refers to the application of a rigid or semi-rigid support, called a splint, to stabilise an injured bone or joint. This procedure is performed to immobilise the affected area, minimise pain, prevent further damage to blood vessels, nerves, or muscles, and make transportation of the casualty safer. Splints can be improvised using materials such as wood, cardboard, rolled-up magazines, or commercial plastic, metal, or inflatable materials. They should immobilise the joints above and below the fracture site whenever possible.
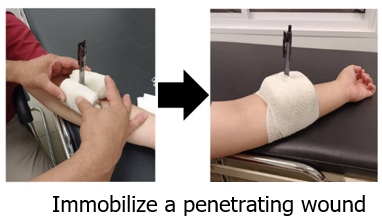
5.4 Immobilisation of a penetrating wound
A penetrating wound occurs when a sharp object, such as a knife, glass, or metal, pierces and remains lodged in the body. In such cases, the object must never be removed by non-medical personnel, as it may be controlling bleeding by pressing against blood vessels or tissues.
Immobilisation involves securing the object in place to prevent movement, which could worsen internal damage or bleeding. This is usually done by carefully padding around the object with bulky dressings, cloth, or bandages, and then firmly bandaging them to keep the object stable without applying direct pressure on it. The goal is to keep the object from shifting during transport, reduce pain, and protect surrounding tissues until professional medical care is available.
5.5 Steps-by-steps to Manage Fractures and Dislocations
As discussed earlier, managing fractures and dislocations shares similar principles and techniques. These are the procedures for managing fractures and dislocations:
- Ensure scene safety & do a primary check (DRSABC).
- Call for emergency help if severe (heavy bleeding, obvious deformity, exposed bone, loss of pulse, suspected spine injury, severe pain, or inability to move the victim).
- Keep the victim still and reassure them.
- Encourage them to stay as still and calm as possible to avoid further damage and pain. Support the injured limb in the position found and do not try to move it unless necessary for safety.
- Expose and inspect the injury (without moving the limb). Look for deformity, open wounds, bleeding, bone protruding, swelling, and skin colour. Check circulation, movement, and sensation distal to the injury (can they wiggle fingers/toes, is the skin warm and pink?).
- Control bleeding for open fractures, but don’t press the bone back in.
- Immobilise the injury (splint or sling). Use a padded splint placed along the limb and secure it so it immobilises the joint above and below the suspected break.
- Pad all contact points and avoid tying bandages so tight that circulation is cut off. After splinting, re-check distal circulation, sensation, and movement.
- For penetrating objects, do NOT remove the object, stabilise it. Pad around the object and secure bulky dressings to keep it steady, avoiding direct pressure on the object itself. Emergency care must remove and treat the wound.
- For dislocations: immobilise and seek urgent care, do not attempt reduction. Realigning (reducing) a dislocation should only be done by trained clinicians.
- Apply cold compresses for pain and swelling (if there is no open wound). Apply a cold pack or wrapped ice for 10–20 minutes (wrap it to avoid direct skin contact). Reapply as needed with breaks, avoid applying cold to open wounds.
- Watch for and treat shock. Keep the casualty warm, comfortable, and lying down if appropriate, monitor breathing and consciousness, and treat for shock (cover, reassure, rapid transfer to care).
- Arrange prompt professional care and continue to monitor. Transport by ambulance if available. Re-check circulation and sensation after any bandaging/splinting and loosen ties if circulation is impaired (pale/blue/cold or pins-and-needles).
Key Takeaways
- Keep the affected limb still and support it in the position found to prevent further injury and reduce pain.
- Never try to straighten a fractured limb or push a dislocated joint back into place, as this may cause additional damage.
- Use a cold compress or ice wrapped in cloth to help minimize swelling and pain, avoiding direct contact with skin.
- Check for numbness, color changes, or decreased movement beyond the injury, and arrange urgent medical attention.
